
Mental Health in Connecticut
Why are we looking at mental health in Connecticut during the Covid-19 pandemic?
Over the past few years, Covid-19 has caused financial, physical, and mental distress among the residents of Connecticut and the rest of the world. Recent research has found that anxiety levels, depression, and overall mental health have deteriorated during the pandemic, with certain demographics of our population experiencing elevated risk.
In this data story, we analyze data from the 2020 Behavioral Risk Factor Surveillance System (BRFSS), the 2021 DataHaven Community Wellbeing Survey, and the 2020 Connecticut Community Readiness Survey to dive deeper into the state of mental health in Connecticut. Important notes and caveats about these data sources can be found in the Data Sources section at the end of this data story.
Happiness, Satisfaction, and Purpose


Higher levels of happiness and satisfaction were associated with increases in age, educational attainment, and income. Towns in the wealthy and rural categories had the highest happiness and satisfaction levels, while urban core had the lowest.
While 70% of respondents overall strongly agreed or agreed that they lead a purposeful and meaningful life, differences were observed within subpopulations.

Overall Mental Health
CWS covered several separate mental health questions on anxiety, interest and pleasure in doing things, and depression.


We observed a disparity in anxiety levels by income level. In general, higher anxiety was associated with lower incomes.


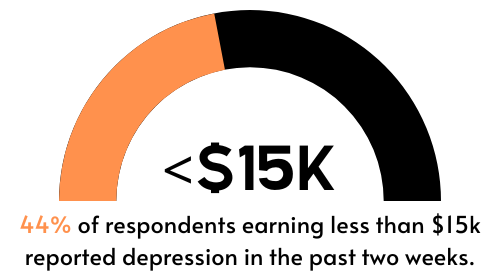
About 1 in 3 reported at least one day of having little interest/pleasure in doing things in the past two weeks. When asked about feeling down, depressed, or hopeless in the past two weeks, data shows that responses were similar to the data on anxiety. In general, higher reports of depression were associated with lower incomes.

Trends in the CRS show that the largest mental health concern for residents 12-17 years is anxiety, compared to depression for all other age groups. Additionally, while the concern of trauma decreases (as the mental health issue of greatest concern) with age, concerns of suicide increase.
BRFSS asked about poor mental health (including stress, depression, and problems with emotions) in the past 30 days.



Depressive Disorder History
In Connecticut overall, 10% of residents indicated that they have been diagnosed with a depressive order (including depression, major depression, dysthymia, and minor depression). However, there was a large amount of disparity between different groups of residents.





Conclusion and Looking Forward
Data indicate disparities in mental health during the Covid-19 pandemic across demographic and socio-economic groups in Connecticut.
Mental Health in Connecticut
In CT, while youth and ethnic and sexual minority populations show a higher prevalence of anxiety and depressive disorder history during the Covid-19 pandemic, key informants also identified a higher level of community concern regarding depression in older adults (66+).
What are some of the potential explanations?
The mental health disparities we saw during the pandemic may be attributable to the long-existing structural-level disparities in our society as well as disparities in access to mental health resources across different racial/ethnic, income, gender, and age groups. Covid-19 isolation and access issues may have worsened existing disparities.
What is the purpose of this data story?
The purpose of this data story is to raise awareness of mental health issues in Connecticut and shed light on mental health disparities, with the hope that state partners can collaborate to address them.
What are some of the limitations?
The limited data on the LGBTQ+ population as well as limited community-level data creates a gap in data necessary to fully understand the impact of Covid-19 on mental health for the state’s most vulnerable populations. Also, state and local data on mental health is still somewhat limited compared to data on other areas of behavioral health.
A push for expansion of data collection on mental health, including risk and resilience factors, is a key next step, as is the development of a data story focused on youth, one of CT’s most vulnerable populations, and one most affected by Covid-19.
Data Sources
2020 Behavioral Risk Factor Surveillance System
The Behavioral Risk Factor Surveillance System (BRFSS) is the nation’s premier system of health-related telephone surveys that collect state data about U.S. residents regarding their health-related risk behaviors, chronic health conditions, and use of preventive services.
We disaggregate by race/ethnicity, sex, education, age, and sexual orientation throughout the data story.
2021 DataHaven Community Wellbeing Survey
The DataHaven Community Wellbeing Survey (CWS) traces its origins to a series of grassroots and locally-based efforts conducted over the past two decades to gather information on well-being and quality of life in Connecticut's diverse neighborhoods.
This data story only displays CWS data for populations that identify as white, Black, and Hispanic race/ethnicity. Data on other race/ethnicity groups are available from DataHaven on request or in its published reports.
2020 Connecticut Community Readiness Survey
The Connecticut Community Readiness Survey (CRS) is developed by the Department of Mental Health and Addiction Services Center for Prevention Evaluation and Statistics and UConn Health. The following are several, but not all, of the goals of this survey:
Assesses perceived substance use problems at the local level.
Measures community readiness for substance abuse prevention.
Informs substance use prevention planning and mental health promotion at state and regional levels.
Identifies needs for training and technical assistance.
Notes
Happiness: Overall, how happy did you feel yesterday?
Satisfaction: Overall, how happy are you with your life nowadays?
Purpose/Meaning: I lead a purposeful and meaningful life.
Terms used within the report represent the terms used within their respective surveys. Examples include terms such as sex, gender, straight, gay, and bisexual.